This week - from skin care to going under the knife, we’re lifting the lid on the science of looking good. Plus in the news, a DNA repair kit that can fix genetic diseases and a UK project launches to clean up 7000 tonnes of space junk.
In this episode

00:49 - Editing the mitochondrial genome
Editing the mitochondrial genome
with Dr Payam Gammage, University of Cambridge
Scientists in Cambridge have developed a system to fix a class of devastating genetic diseases called mitochondrial enzyme defects. They occur when structures called mitochondria, which supply our cells with energy, don’t function properly. This happens because some of the mitochondria, which contain their own small piece of DNA, carry genetic changes or mutations that prevent them from working properly. Now there might be a way to fix the problem: Payam Gammage from the Medical Research Council’s Mitochondrial Biology Unit at Cambridge University has developed a gene editing system that knocks out selectively the defective mitochondria so they’re replaced by healthy working ones. Payam spoke to Katie Haylor...
Payam - Severe mitochondrial diseases are likely to result in the patient not often leaving the hospital, serious mobility problems, they’ll likely have cognitive difficulties requiring round the clock care most of the time. And life can really be very very difficult, and in slightly less severe cases being wheelchair bound and struggling to live an independent life.
We aimed to develop a system that would enable us to target the mutated mitochondrial DNA and take that percentage down from, say 90 percent mutated down to 50 percent mutated. Then hopefully, someone who did have the clinical disease no longer has it any more.
Katie - So you’re talking about editing someone’s genes?
Payam - We’re talking about selectively removing one entire subpopulation, yeah.
Katie - So how on earth do you do that?
Payam - We took some genome engineering tools, which had been developed in a different form for different purposes: zinc fingers - zinc finger nucleases to be precise. And what these things do is allow you to do is target specific portions of DNA and cut it. If you cut the mitochondrial genome it gets degraded, and so if you can selectively cut the versions of the mitochondrial genome that have a mutation. Then you selectively remove them from the total pool and so hopefully you change the percentage of mutated versus healthy.
We created these zinc fingers that would be specific to the mutation in this particular mouse that has a relatively mild form of mitochondrial disease, and it has a mutation which is very similar to a human mutation. We tested it in mouse cells to see if we could alter this ratio of mutated to unmutated and we put it into the mouse. So injecting into the bloodstream the genetic instructions for these zinc fingers using a harmless virus that’s been repurposed for this kind of thing, and this virus really really likes to be taken up by heart cells, predominantly. We measured the levels of healthy mitochondrial DNA versus mutant starting, from about 70 percent and going down to about 30/35.
Katie - So that’s well below the level at which people would show symptoms?
Payam - Yes, yes. Well below the threshold. Cells generally like to maintain a total number of mitochondrial DNA molecules, so say it’s a thousand. If we’ve removed say 20 percent of them or 30 percent of them, what will happen is the remainder will be replicated. And so basically, every time you remove one molecule you’re increasing the chance that it will be replaced by a healthy one.
Katie - How far are you away from doing this in humans?
Payam - The beauty of this approach is that its generalisable. So every time we want to target a new mutation all we have to do is re-engineer the parts that bind DNA and then it’ll work. That will take us a certain period of time; a few months perhaps to design some new ones to human mutations and then to get ourselves into a position to be performing clinical trials in humans - that could take a little bit longer. We’re hoping to have something on the cards within the next year or so.
Katie - Are the mutations in people who suffer from mitochondrial disease different from each other and, if so, do you have to personalise this tool for every single person that you treat?
Payam - There is a pretty broad selection, yeah, of mitochondrial mutations that occur in humans and cause disease. But there are some real standout candidates that appear much more commonly than others; for example there’s one which counts for about 30 percent of all mitochondrial DNA mutations in humans. So there is definitely going to be a required level of re-engineering for different people in a personalised medicine kind of approach, but a good proportion of the population should be served by a handful of these therapies.
Katie - You’re just doing this with mitochondrial DNA, are there any risks to the nuclear DNA?
Payam - We can’t find any evidence of any activity of what we’ve developed in the nuclear genome. We took parts of the nuclear genome that looked very very similar to the area in the mitochondrial genome that we were targeting, and then we assessed the area around it to see if anything had changed, and in our experiments where we did this we found absolutely no changes.
In a world where you don’t have an effective treatment it’s a potential silver bullet. Obviously, there’s a lot of caveats that go with that and a lot of optimisation and careful testing and safety assurances. It potentially, is a very very big step change for people who suffer from these diseases.

06:02 - Labelling learning difficulties
Labelling learning difficulties
with Dr Duncan Astle, University of Cambridge
Now the school term’s begun here in the UK, and all over the country kids are going back or starting school. Some children have the extra challenges of learning difficulties to contend with, and might have been diagnosed with conditions including attention deficit hyperactivity disorder or ADHD, dyslexia, or an autism spectrum disorder. But how helpful are these categories for kids who are struggling at school? Using machine learning, Cambridge scientists have studied hundreds of children with these diagnoses, and identified clusters of learning difficulties which did not map to the diagnoses they had received. Chris Smith spoke to cognitive neuroscientist Duncan Astle, who led the study. Firstly Chris asked Duncan why the team did this study...
Duncan - Well, many children struggle with learning. There’s disorders like ADHD which was mentioned, so prevalence rates for those kinds of those things vary from 3 to 8 percent. But, actually, the proportion of children who struggle to learn is much higher than that. Governments statistics are around 30 percent of kids don’t meet their age expected levels by the end of primary school.
We’re really interested in what are the underlying causes or the underlying roots to being a struggling learner. And the way that you would normally study that would be to choose a group of kids that you’re interested in, say kids with ADHD and you would compare them to all the kids who don’t. But we began to think that there was some real problems with relying solely on that approach. The first one is that it assumes who have the same diagnostic label are all the same as each other.
Chris - You're genuinely comparing apples with apples but they actually might not be?
Duncan - That’s true.
Chris - Yeah. So who did you recruit then?
Duncan - Well, we set up a centre which we called the Centre for Attention Learning and Memory and to that centre professionals in education, in clinical services could refer children to us that they thought were struggling. They didn’t have to have a diagnosis but they could, or they could have multiple diagnoses. They just had to be struggling in the areas of attention, learning, or memory, so intentionally generic.
Chris - And how did you study them?
Duncan - Each family would visit us and the team of research assistants and PhD students would spend several hours doing different kinds of cognitive assessment with the children. And we would have behaviour ratings for the parents to fill out and most of the children would go through the MRI scanner.
Chris - So you’ve got what their performance is like, what their performance is like as in their track record, what their performance is like in your tests and a brain scan to go with. And what, you then marry all that information, or at least you’re asking a computer to marry all this information together and look for common ground or differences between them?
Duncan - Essentially, yes. We took many of the cognitive assessments and we fed them into a machine learning algorithm. Machine learning sounds kind of fancy, but actually we use it all the time in our everyday lives. Every time you type something into a search engine, behind the scenes there’s an algorithm which is learning about that information you’re feeding it, and you might notice that appear in your adverts that correspond to what you’ve searched for. Our machine learning algorithm was learning about the cognitive data that we fed in from these kids and what it learnt was that there were different profiles for children. Children with different profiles of cognitive difficulty.
Chris - What does that mean in practical terms? When you say different profiles are you saying say I had a diagnosis of ADHD, I’ve got that label but actually my ADHD may be quite different from the label of ADHD you might receive, for example?
Duncan - Yeah, exactly. Because one thing we could do is then check about what the machine learning algorithm has learnt and see whether it’s really learnt the categories, the diagnosis the kids came with. And the data showed very clearly that’s not what the machine learning was learning. Children who had a diagnosis of ADHD could have very different profiles from each other. They could have very different cognitive strengths and difficulties and that’s a real challenge in trying to think about how we support those kids.
Chris - Does this mean then our categorisation is just wrong? We’re putting people into narrow bins of problems and, in fact, it’s much more subtle than that and we need much sort of narrower but wider categorisation?
Duncan - I think it means the diagnoses, we’re not thinking about them in the right way. So they’re not like kind of medical diagnosis, they’re much less discrete and clean than that, and we don’t really understand what the underlying causes are. We still think that a diagnosis is a real landmark moment for children of families when they get some professional recognition for the challenges they’ve been facing. The question is how do practitioners then best support those kids, and how do we equip those practitioners to do that? And the answer is simply knowing the diagnostic label itself isn’t enough information to go on.
Chris - Indeed. At the end of the day we’re dealing with an individual here that’s got a problem that they want help solving isn’t it? So does your tool give us a better insight into okay, we can identify where this person’s weaknesses are so we can then go to the classroom and say if you augment the training in this direction, or give this person extra aids, perhaps more stimulation, more practice in this area this will help to develop this area that they are clearly deficient in?
Duncan - Well, we believe so. So, for example, in the data a large proportion of the children have problems in short term or working memory. Those children could have a diagnosis of ADHD, they could have a diagnosis of ASD, or they could have no diagnosis at all.
Chris - Autism spectrum disorder?
Duncan - Autism spectrum disorder, or they could have not diagnosis at all. But we know that if you try and reduce working memory demands in the classroom, then kids with poor working memory will do better. We already know that there are some interventions out there that are effective with these kinds of cognitive difficulties, it’s just that they seem to cut across the traditional diagnostic boundaries that we’ve kind of hitherto believed in.

12:54 - Scooping up space junk
Scooping up space junk
with Professor Guglielmo Aglietti, University of Surrey
Imagine saving up for years to buy a new car but, to get it home, you first have to drive it through a pile of old metal meaning you end up take the side off it in the process. That sounds far-fetched but it’s effectively what’s happening to the new satellites we’re sending up into space, because the planet is surrounded by a sea of orbiting junk left behind from our previous forays aloft. And this rubbish is threatening to jeopardise technology worth millions! Now scientists across Europe are taking this bull by the horns with an imaginatively-named project called RemoveDebris. Izzie Clarke spoke with Surrey Space Centre Director and leader of the project Guglielmo Aglietti...
Guglielmo - Currently there are more than 7 thousand tons of stuff up there in space and mostly are old satellites or the final stage of rockets. Things that have been put in orbit maybe decades ago and they are still there spinning around. Some of them have broken into bits. It is a problem because this stuff in orbit travels really fast and so even as more fragment hitting another satellite could destroy this new satellite.
Izzie - Imagine spending all that time researching a brand new satellite only to launch it into orbit and then have it destroyed by a piece of space junk. Well, Guglielmo and his team are planning to change all that…
Guglielmo - Well, what we have done with our partner is to put together a consortium to demonstrate the technologies that can be used to remove some of this debris and the project has been sponsored by the European Commission. The kind of technologies that we are going to demonstrate are relatively simple technologies if you want.
One is a net. The idea is to capture your piece of debris with the net and this net envelopes the object and then you can drag it down. Another technology that we are going to demonstrate in a few months is a harpoon. Also here is a similar thing so with the harpoon you try to capture your object and then you will pull it down until it burns into the atmosphere.
Izzie - Okay. So you’ve just done this first test so talk me through it. How did it work?
Guglielmo - Okay. Everything went very well. From the main satellite, which is the size of an old television set we have released our artificial target. It’s maybe the size of a loaf of bread to give people an idea. Then this has inflated a structure to be much bigger so it is more representative of a real piece of debris. Then from the main satellite we have launched the net that has captured our little debris with this inflatable structure and has completely enveloped our debris. And so now is going to the orbit with it and burn into the atmosphere.
Izzie - How is all of this controlled? How would your device know where to capture this piece of debris?
Guglielmo - Ah, well. In our case we have released our own piece of artificial debris so we knew where it was, and therefore was relatively easy to recapture it. In a real scenario the first thing that the satellite will have to do is to get closer to the potential target, so you would have to have a more sophisticated control of the satellite in order to get closer to your target; therefore you can capture it.
Izzie - Another test that the RemoveDEBRIS team has scheduled is to use a camera to monitor the speed and shape of debris in order to track how a potential target moves. After that it’s over to trying a harpoon rather than a net to capture this junk. But how does it all then get destroyed?
Guglielmo - The idea is that we are going to lower the orbit so this junk can burn into the upper atmosphere. And normally our satellites are designed in a way that they can burn completely in the higher atmosphere. However, you will try to do these maneuvers maybe over the ocean so even in the unlucky case that a little part of your satellite maybe doesn’t burn completely, the potential fragment then drops into the ocean rather than in an area where maybe there is a higher density of habitants.
Izzie - Rather than trying to scoop up every bit of space junk this debris harvesting device will aim to collect the biggest pieces of junk in space to save them from breaking up into smaller fragments and adding to the overall pile of debris in orbit. Once it has been scooped up the net or harpoon, the RemoveDEBRIS satellite will use a giant sail to steer towards our atmosphere until the satellite, and the junk in tow, is all burnt up. So what's next for the team?
Guglielmo - Now that we have shown that the technology is viable we hope to be able to convince all the stakeholders to actually finance such a mission. What we imagine is just to do a few missions every year where people would agree beforehand what is the particular piece of debris that we are targeting so you can go up and capture this piece of debris and then deorbit it.This is the kind of scenario we have in mind.

18:32 - Wearable tech: sensing when you've had enough sun
Wearable tech: sensing when you've had enough sun
with Professor Vipul Bansal, Royal Melbourne Institute of Technology
Basking in the warm sun is a luxury that many of us love, and it’s also good for you - up to a point - because the ultraviolet rays in sunlight produce the bone-boosting hormone vitamin D in your skin. But too much UV causes sunburn, skin ageing and wrinkles, and it’s a major risk factor for skin cancer, rates of which have more than doubled in recent decades. Now scientists from Australia have come to the rescue with a wearable sensor that you pop on your wrist; it goes blue when you’re past the safe daily sun limit for your skin type. Inventor Vipul Bansal told Tamsin Bell how it works...
Vipul - UV is invisible and it’s not hot so you can’t feel UV, and the heat that we feel in the sun is because of infrared rays, it’s not because of UV. We are trying to make UV sensors in the form of wearable sensors which change colour when you go in the sun. This ink can interact with the UV light and then become blue.
Tamsin - So once our sensor becomes blue we know that we have to go inside?
Vipul - Yes. And this ink can give a warning signal - now it’s time for you to go back in.
Tamsin - How does this work? What chemicals are involved?
Vipul - The two main chemicals in this ink - we call it an invisible ink because it’s initially colourless. There’s a chemical called polyoxometalate that's a big molecule, a lot of phosphorus, oxygen involved. The second component in the ink is lactic acid, a common chemical which is present in yogurt. So when we mix these two components together and we shine this ink with the UV light, the lactic acid molecules can give electrons to the other molecule. When this happens the polyoxometalate becomes blue in colour and that’s what we see.
Tamsin - What about different skin types or UV tolerance, how does this take that into account?
Vipul - We have six different types of skin. It could be very fair skin to very dark skin. Now the UV requirements and the tolerance of these skin types are very very different. The very fair skin cannot tolerate a huge amount of UV; if you look at a darker skin it can tolerate a reasonably large amount of UV, which means that we have to have personalised sensors for different skin colours. So a sensor that would be for very fair skin, it should develop colour very very fast. On the other hand the colour should develop slowly in case of a darker skin, so a person can stay in the UV for a longer period of time.
Tamsin - I’m a bit of sun worshiper. Is this sensor going to tell me that I have to stop sitting in the sun really quickly?
Vipul - A lot of us love sun and we cannot really avoid exposure to sun. We are recommended to use sunscreen with a high SPF number to reduce the amount of UV that is reaching your skin. When you are applying the sunscreen on your skin, you can also apply it on the sensor. It will also reduce the amount of UV that reaches the sensor and the sensor will develop colour slowly.
Tamsin - I suppose the same would apply if someone sat in the shade?
Vipul - Yes, that is true. We call it a cumulative dose. So when they are in the sun then only the sensor will work and depending on the intensity of the sun the sensor will either work faster or slower. And then it won’t go back once you go back into the shade, so in that way the sensor lasts for one day. We see a huge prospect of these sensors because the sensor can allow people to be exposed to the maximum dose possible without causing harm.
Tamsin - Are you planning to make these and sell them in shops, and how much would it cost?
Vipul - We have a very ambitious target to bring it to the market by early 2020. The retail cost would be somewhere around 1 dollar.
10 years of the LHC
with Professor Tara Shears, University of Liverpool
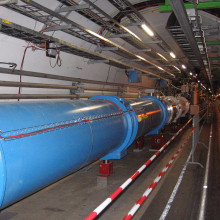
10 years ago this month, the Large Hadron Collider switched on for the first time, and began its quest to revolutionise our understanding of the universe. But how successful has it been? Adam Murphy...
Adam - Under the ground near the Swiss/French border lies the Large Hadron Collider or LHC. A 27 kilometre long ring; one of the largest engineering projects ever undertaken. It was built to help us unlock some of the fundamental secrets of the universe. But how does it do that? Tara Shears is a Professor of Particle Physics at the University of Liverpool…
Tara - Somebody described it as working out how a Swiss watch works by bashing two really expensive ones together and trying to reconstruct what’s in there from all the bits that fall out. It takes two beams of protons, which are hydrogen nuclei, and it circulates them in opposite directions around this ring, and it accelerates them until they’ve got loads of energy, until they’re travelling just a few metres per second less than the speed of light. And then those beams are steered to smash together at four points around this ring where we build our experiments.
And it’s what goes on when those beams crash together which is the key to our whole investigation because when those proton beams smash together what’s actually going in is the tiny tiny instance of time, the tiny area of space, we have so much energy that we can dissemble matter to its fundamental constituents, and we can make new fundamental constituents from that energy. And our experiments act as gigantic 3D cameras and take snapshots of the traces these particles leave behind when they zip out from the collision point and deposit their energy throughout all our detector material.
Adam - Probably the most famous result of the LHC is the discovery of the Higgs Boson for which François Englert and Peter Higgs were awarded the Nobel Prize in 2013.
Tara - The Higgs Boson is an absolutely integral part of the universe. Well actually, the integral part of the universe is something called the Higgs field. It’s a type of energy field which is present throughout the universe. And the reason that this is such a big deal for us is that we think it’s this field, and the interactions that fundamental particles have with this field as they move around the universe that gives fundamental particles their mass. Which might not sound like a particularly big thing but it’s absolutely necessary for us to be able to make sense of the way particles behave, of the way the forces govern particle behaviour have their particular strengths. And this field, and the particle, the Higgs Boson that’s associated with this field is an absolutely integral part of our theoretical understanding of what’s going on.
The LHC was designed so that if the Higgs Boson existed, then we should be able to see it. And indeed, back in 2012 we did see the first observation of this particle, and then ever since we’ve been gathering more data.
Adam - What has the discovery of the Higgs meant for science?
Tara - What the discovery of the Higgs Boson did for us is it filled in the missing parts in our current understanding of matter. It’s like having a jigsaw and getting those last pieces and sticking it in, and then all the pieces lock together and you’ve got a coherent picture. You know, you can see it in front of you; it works; it’s brilliant. You can’t overstate what an important step forward that was.
Adam - And the LHC’s work is far from finished…
Tara - As well as being constructed to try and find the Higgs Boson, the LHC is really a discovery machine. Although we’ve been going 10 years, we’ve only taken about 5 percent of our ultimate dataset. The LHC is a real long term machine. We’re thinking that it will carry on until 2035, maybe even a little bit longer, so there’s an awful lot more data to come.
So if you think what we’ve already done with the 5 percent of data that we’ve got with the discovery of the Higgs and all these other investigations that have told us more about the limitations of our theory, and the limitations of our alternative hypotheses, I can’t tell you what’s going to come out of the next 95 percent. This is the thrilling thing about doing research. The data that we’re collecting tells us something new and I’d be foolish to try and guess what’s out there.
Adam - What was it like to be a particle physicist that first day ten years ago?
Tara - Oh, it was just amazing to see the evidence for this first beam go round. It was quite awe inspiring actually when you think of all the engineering, all the design, and all the work that had gone into this machine and yet it worked when they switched it on.
I still find that incredible. It’s a massive endeavour. There aren’t many massive endeavours on this scale. For us, it’s almost akin to the Moon landings and the space race in terms of going out there and finding out what there is. It’s another one of these endeavours of mankind that make you think that mankind at heart is brilliant if it can do this sort of thing.

28:30 - Why bother looking good?
Why bother looking good?
with Professor Viren Swami, Anglia Ruskin University
From cosmetics to clothes, to going to the gym, most of us pay attention to our physical appearance. But why? To find out, Katie Haylor spoke to social psychologist and body image expert Viren Swami from Anglia Ruskin University. First Katie asked Viren, why bother trying to look good?
Viren - There are a number of different theoretical explanations. The kind of the most dominant one is the evolutionary psychological one that we try and look good because you want to attract mates. And the way we demonstrate our health and fitness is primarily through our attractiveness. The idea is that attractiveness is highly linked with health and fertility and that people who look attractive are more fertile and healthier. So we try and demonstrate our effectiveness or our propensity to mate with other good looking people by demonstrating our own attractiveness.
There is also a cultural explanation, which is simply that we are generally biased to perceive attractive people as having better personal qualities. Being more sociable, being happier, being better at work, and all kinds of other personal qualities. And if you have that bias or if you incorporate and internalise that bias, then you want to look good because you think you’ll accrue the rewards of looking good.
There is also a neuroscientific explanation, which is that our brains process attractive people as more rewarding. There is part of the brain called the nucleus accumbens, which shows heightened activity any time we see attractive people. And the suggestion from neuroscience is that our brains like it when we see attractive people so we try and demonstrate our own attractiveness.
Katie - Now, I’ve made a bit of an assumption that everyone pays attention to how they look. Is that true?
Viren - There is evidence to suggest that most people pay attention to how they look but also that they conform to different standards of grooming. So most people have an idea of what’s expected of them societally in terms of what they should look like, whether it’s in an occupational settings, or romantic settings, or in daily life.
They also have an expectation of what they should look like in terms of their grooming but there are also individual differences. So, for example, there are studies suggesting that people who are higher in what we call “appearance investment” tend to spend more time focussed on their appearance, and also tend to believe that their own appearance has a huge impact on life outcomes; whether they get a job or whether they’re likely to find a dating partner and so on. People who are low in investment appearance tend to think that appearance isn’t particularly important and they consequently spend very little time on their own appearance.
There are also other factors that might relate to how important you think appearance is, and also your use of cosmetics, for example. There is some evidence to suggest that people who are, for example, higher in what we call “oppressive belief” so people are more sexist, who are more hostile towards women, are more likely to believe that women in general, but also their partners, should use cosmetics.
Katie - So, in my handbag, which is sitting in the corner of your office, I’ve got some mascara, some foundation, some lipstick. I’m probably not alone. Why do so many of us paint it on our faces?
Viren - I think there are a number of reasons. If you look at it from a cultural point of view, particularly for women, I think there is pressure to conform to stereotypes of what femininity is. At the individual level, the reasons might be very different to why someone might choose to use cosmetics compared to the political or the social level. There is a good deal of data to suggest that when women wear makeup they feel better about themselves. When women wear cosmetics they feel more confident, they feel more self-competent, and the also perceive themselves experiencing better rewards as a result.
Katie - And have the same studies been done on men or people of other genders?
Viren - Not at the moment. We know very little about men who use cosmetics and particularly men who use makeup. There is evidence to suggest the use of makeup among men is increasing, but we don’t know necessarily about the outcomes. One of the difficulties with men and cosmetics is that, historically at least, the use of makeup in men was considered transgressive in terms of their masculinity. More recently, there is evidence to suggest that the use of makeup has been incorporated into some forms of masculinity.
Katie - What about other people’s opinions of us then? Can, for instance, wearing makeup may change the way someone else might behave towards me?
Viren - Again, it’s really difficult to know whether they’re responding to you because of the makeup or because they perceive you as being more attractive. I think there are two separate things here. I think one is the kind of general response from other people. It’s quite possible that the responding, for women particularly to you using makeup, because they perceive you as being more feminine as opposed to when you don’t use makeup when you’re perceived as being less feminine. So there are lots of interactions between the perceptions of people based on whether or not they’re using makeup.
There are also studies suggesting when women wear makeup they’re perceived as being more competent, particularly for high-powered jobs. Because again, it’s consistent with the perception of what’s required for those jobs. So it’s really difficult to know whether the response at the level of the general population is to you because you’re wearing makeup, or because you’re conforming to societal normal about what you should and shouldn’t do.
Katie - So if I go to a job interview and I put on some makeup, is that really going to increase my chances of getting the job?
Viren - It turns out it is possible. And it’s certainly likely that you increase the likelihood of you having a successful outcome from that job interview, but I suspect this is partly a function of the people who are interviewing. Historically, at least, job interviews tend to be dominated by men and they have certain expectancies about what they would like and don’t like women doing. And the assumption here would be that women who wear makeup are kind of conforming to a gender role and men feel more comfortable when women conform to that gender role.
Women on interview panels might be doing the same thing. So they might be assuming that when other women are coming for a job are conforming, they feel better and safer around these women.
Katie - And there’s evidence to backup that notion?
Viren - Yes. The other really interesting thing is how a partner might respond to you. And this is particularly true of men’s responses to their female partners in heterosexual relationships. There is some evidence to suggest that when heterosexuals are in committed relationships men generally don’t like their partners to wear makeup. And this might be because they perceive it as a means of attracting other partners so they experience greater feelings of jealousy.
One of the nice things about social psychology is that we also know that the importance of first impressions drops off very quickly. So the importance of physical appearance matters most in the absence of any kind of social interaction so when you see someone for the very first time you make a judgement about that person based on their physical appearance alone and that makes sense because you’ve got no information about that individual.
Once social interaction begins, and this is also true of interviews and job interviews and so on, also romantic relationships for example, once you begin to have social interactions you begin to piece together a much fuller picture of the individual and you’re kind of gleaning much more satisfying and richer data. And you begin to use things like reciprocal information, whether you’re exchanging information with the other person, or whether you’re exchanging intimacy, whether you’re exchanging useful information with the other person in a job outcome, things like similarity also then begin to matter then as well.
Kind of the key point is that although appearance really is important, particularly in occupational settings, the importance is often overestimated.

Cancer risk and breast implants
with Dr Suzanne Turner, Cambridge University
More extreme than wearing makeup is resorting to surgery to alter your appearance. And one currently very popular body modification is breast augmentation. This involves inserting bread-roll-shaped implants filled either with a silicone gel or a saline solution underneath the breast tissue to make the breasts look larger. People say that it gives them more confidence and satisfaction with their body. But, the procedure has since been linked with an increased risk of developing a cancer of white blood cells called anaplastic large cell lymphoma or ALCL. Chris Smith spoke to Cambridge University’s Suzanne Turner - one of the team that discovered this. First, Chris asked Suzanne how common breast implant surgery is...
Suzanne - About 6 to 10 million per year.
Chris - Oh, huge numbers.
Suzanne - Huge numbers, yeah.
Chris - Okay. And this condition, how did it first come to light?
Suzanne - The first case was reported back in 1997 now. And this was a case that was in the literature but not much attention was paid to it to begin with.
Chris - Tell us about the disease then. When someone has ALCL what have they got? How would they know they had it?
Suzanne - It’s generally a sudden swelling normally in just one breast, which can come on anything from one year to over ten years past surgery. That swelling tends to stay around; it can also come as a lump either in the capsule that forms around the breast implant. This is an area of fibrous tissue that forms in response to the breast implant and lumps and bumps around that area can also be a sign of ARCL.
Chris - Is it painful or painless?
Suzanne - Both. Women have reported all sorts of ranging symptoms associated with this.
Chris - Interesting. So the disease actually happens locally to the implants happening but one side, both sides?
Suzanne - Generally one side. Generally there’s just one side involved.
Chris - So what do we think the mechanism is then that encourages this particular tumour to form?
Suzanne - There are a number of theories out there. The first one that it’s infection driving this so during the surgery perhaps some infection gets involved, and this lingering infection leads to the white blood cells proliferating out of control and becoming this lymphoproliferation - this cancer.
Another theory is suggesting that some women may be allergic to these breast implants and this allergic response, which goes on for a long period of time, again drives these cells into proliferation.
An alternative theory is that for some women there may be an autoimmune condition that predisposes them. So it may be the case that they already have an autoimmunity and the presence of the implants upsets the balance of white blood cells within their body.
And, of course, the theory we can’t really discount is the breast implants themselves. And are there toxins related to those breast implants, for example, which may also be driving this form of disease? And, of course, we know for many cancers there could, in some cases, be a driving toxic stimuli.
And, of course, breast implants are made of a whole array of different chemicals that we don’t really know too much about. How these are manufactured is a closely guarded secret by the companies that make them.
And so I think all four theories aren’t necessarily mutually exclusive. I think that there may be a multitude of mechanisms towards this particular cancer and that for some women they may be at a higher risk than others due to predisposing conditions.
What we do know is it’s mostly associated with women who have a form of implant that has a textured surface. This is a very specific type of implant that’s been introduced as a way to deal with something called capsular contracture, and this is where the fibrous capsule that forms around the breast implant can pull the skin in forming a sort of dimpling effect. So these textured implants have certainly been more commonly associated with this form of cancer.
Chris - The thing is though, we put lots of other implants into the body. People have hip replacements, other joint replacements and other things put into various places. Do they carry the same risk because many of the mechanisms you’ve outlined do not strike me as being unique to what we do with breast implantation and breast augmentation surgery?
Suzanne - Absolutely. You’re right there so you would expect that if it’s bacterially driven and it’s due to the surgical procedure in itself, you would see these lymphomas occurring in people with all sorts of other implants, and actually you don’t. There are some rare cancers that have been associated with metallic implants but, for the most part, we only see breast implant associated ALCL with breast implants so I think that gives us some clues as to what’s really driving this.
Chris - And just very briefly, what’s your overall risk then? Because there may well be people listening to this if they’re one of that, you know, very large cohort - millions of cases a year having breast augmentation, what’s your risk of having this condition?
Suzanne - It is rare. But the risk in the UK is currently placed at 1 in 28 thousand women with breast implants and that’s data based on the number of implants that are sold, although of course, we don’t know how many of those implants actually make it into women. Although, if you read through the literature the rates of this disease developing range from 1 in 3 thousand women with a textured implant to 1 in 30 thousand women. So there’s a whole array of different rates depending on where you live and which literature you read.
Chris - So if you’re in one of those unlucky groups who is diagnosed with this, Suzanne, what can you do about it?
Suzanne - The treatment is fairly straightforward for the ladies that are diagnosed very early on in the disease. The treatment is literally the removal of the breast implant and the capsule that surrounds the implant and, for the majority of these women, that’s enough to put the disease into remission.
However, having said that obviously it is a surgical procedure and it’s not something that anybody would enter into lightly. And, at the same time, there are the implications of whether or not to have a replacement implant and whether or not that is safe and, unfortunately, we still don’t really know. Some women are having smooth implants put in in place of the textured implants, but I don’t think that the evidence is fully out there yet that the smooth implants are any safer necessarily.
Unfortunately, for some women, these cancers do develop and they do progress into something more, and for some rare women, this can be the first sign of the cancer. I’m aware of ladies who’ve had masses growing into their rib cages with a very aggressive disease that needs chemotherapy.
So it can be a very aggressive, nasty disease and there have been about 16 deaths reported worldwide, so it’s not something which should be looked upon too lightly.
Chris - Do you think on the balance of it that, actually, the ends justify the means? Do you think we should still be allowing people to have breast implants given that they are effectively taking a risk? It’s not just a one in a million chance, these numbers are quite high the risk that you’ve been saying of this happening.
Suzanne - It’s very much a personal choice, and I think at the heart of it all is that women should be able to make an informed decision. And up until a few years ago that was not the case, women were not being told this was a risk. So now that we do know that it is a risk, it’s very important that plastic surgeons convey this risk to the ladies before they make the decision as to whether or not to have implants.

42:50 - The chemistry of cosmetics
The chemistry of cosmetics
with Dr John Emsley, chemist and science writer
What's in the creams and powders that many of us put on our faces? Chemist and science writer John Emsley spoke to Katie Haylor. First up, Katie asked John, what's actually in the lipstick she puts on her lips?
John - Well, what you’re putting on is something like a wax or an oil mixed together with a colour or a dye with it. There are other components; there are about 20 components in some lipsticks. But basically, you’re doing what Ancient Egyptians did or Ancient Romans did, you want to highlight your lips with a deep red colour. In those first things they were using quite dangerous materials, they were using things like cinnabar, which is deep red but, of course, that’s a mercury compound. Today we use safe dyes and there’s no risk of you being affected by anything that you put on your lips.
Katie - Well, I’m very glad to hear it because I’ve just put some on. Now, I’ve just taken a sip of my cup of tea that I’ve got here in the studio and, unfortunately, I now have purple on the cup.
John - Oh, dear.
Katie - Is this supposed to happen?
John - Well, modern lipsticks were invented about a hundred years ago in America, and there were lots of faults with them to begin with. They were greasy; in cold weather they snapped, broke off; in hot weather they melted. They tended to pick up germs so they very quickly became infected. And, of course, people were using them because they were a simple way of applying colour to your lips.
Well, of course today, all of those problems have been solved. You’ve got a better range of colours. You can make it glossy, you can make it even sparkle by the things you put in it. And, of course today, we’d like to think of the colours that you’re using are impermeable; in other words they won’t pass from your lips to whatever you touch.
I’m afraid to say I’d go round and look for something slightly better if I were you.
Katie - Now secondly, mascara. It’s a common thing to find in the makeup bag. This is put on my eyelashes. What is it?
John - Well again, mascara’s been around since ancient times. And the very first mascaras were using something called kohl. Now kohl again, there were minerals. There was an antimony mineral and there was a lead mineral that people used in those days, but you’re going back now to Ancient Egyptian times again.
Today, of course, they’re much safer. What you’ve got in a mascara is you want a wax base, and some of them actually use beeswax or carnauba wax and things like that. They tend to mix that with an oil so it’s much more flexible than just the simple wax. You also want something that keeps it permanently soft like glycerine, glycerol. You also want other components there, you obviously want a dark component. Today you’d tend to use carbon black or very black iron oxides.
You don’t want, of course, there to be infection in your mascara because you don’t want your eyes to become infected and you’ll need to protection against germs and things like that. So again, it’s a very complex mix but today, I think, they’re about as safe as it’s possible to be.
Katie - So John, another thing I’ve found in my makeup bag is a foundation liquid. What is foundation?
John - Well, the idea of foundation is protect the skin of the face and to mask blemishes. And so, lots of things could be included in foundation. Of course it depends, generally they’re different forms of iron oxides, so you can get the skin tone that you’re looking for. Very often you want to put a silicon layer on your skin because that protects it. It prevents water being absorbed from the skin so this can remain slightly plumper and, of course, it protects the skin against outside influences. So it’s a protective layer and it’s a disguise - that’s basically what a foundation is.
Katie - So John, now we’re in 2018 and a lot of people wear foundation but I’m guessing people have done this throughout history. So, as far as we know, when did people first start wearing foundation and how has it changed over time?
John - Again, we can trace that back to ancient times - mainly upper class women who used it. They didn’t want their skin to appear rugged. If you were an ordinary person and you worked outside a lot then, of course, you’d be exposed to UV, your skin would begin to look aged. You didn’t want to show you were such a person so you wanted a lighter skin, and very often what they were applying to their skin was very light pigments. Sometimes they even used arsenic trioxide, which was known as white arsenic in those days. And I believe Queen Elizabeth I was very partial to having her skin looking very white as proof that she was the upper class woman of the time.
Arsenic on the surface of the skin is not a threat. It does of course if it gets into your body. But even on the tiny amounts that you might have absorbed it wouldn’t do anything dangerous. Then of course sometimes, if you took a little arsenic into your body then you’d get a red blush forming on your cheeks and, again, that was something that women took arsenic for at one time.
Katie - Oh dear! Okay, well I’m certainly not going to be doing that now. A slightly different one John, but what about deodorant and antiperspirant? It’s a cosmetic of sorts if we think about it trying to make us smell nice. What actually are these kind of sprays or roll-ons?
John - They're basically more important for men than women because men tend to smell. They tend to produce a lot more body odour than a woman does. Now you can stop that, you can prevent the bacteria that are producing these odours if you block the pores of you skin in the armpits which, of course, is where lots of the sweat is produced, and so you'd spray on something that would block them. Once it was aluminium salt but that fell out of favour, now it can often be a zirconium salt. You block those pores, you won’t produce as much sweat and so you can go off for the evening.
Katie - Deodorant antiperspirant blocking these pores, is it a good idea? Is it safe?
John - It wouldn’t be safe if you tried to do it all over your body, I mean there are people who’ve painted their body and died very quickly because you’ve blocked every pore. But it’s just these very profuse sweating glands under your arms that then produce these bacteria and then they give off very often sulphur based smells, which are quite strong and that all sweaty odour. And, of course, if you’re going out for the evening you’re going to mix with people, you don’t want people coming up to you and then backing away thinking oh god, what a pong! You want to give off a lovely come hither smell don’t you? Of course for women it’s just as important to do this as well. The other thing about deodorants is you can try and kill the bacteria that are causing it but, again, some of the, like triclosan, some of the very powerful antibacterial agents are now frowned upon. And so it’s perhaps best to shower every day and remain as fresh as you can.

The science of skincare
with Dr Jane Sterling, Addenbrooke's Hospital Cambridge
Many of us spend a great deal of time, money and energy on our skin, but are the various potions and lotions in our bathroom cabinets actually doing it any good? Chris Smith spoke to dermatologist Jane Sterling from Addenbrookes Hospital. First off, Chris asked Jane for the lowdown on skin...
Jane - Well skin, of course, is the covering to all our bodies, with a slightly modified version over the front of the eye and mouth. There are two important layers of the skin, there’s the epidermis, a wonderful self-renewing very thin surface that’s continually being made from below, and continually lost from the surface. And below that is the dermis. That’s the stretchy but sort of padding layer just beneath, and then, of course, we get down to fat and muscle. So our skin is a self-renewing surface. It protects us from the outside and keeps the inside - inside.
Chris - One statistic I read was we lose something like 40 or 50 thousand skin cells every second. Does that sound about right?
Jane - We certainly lose a lot. And most people don’t realise that household dust is mainly skin that’s being shared.
Chris - As we were walking around through our homes you’re breathing yourself and your housemates in. Isn’t that true?
Jane - That is true.
Chris - When the skin is young and youthful, like yours and mine, why is it different from someone who’s gone all craggy and needs loads of lipstick, like Katie - no I’m just kidding Katie, you’re not all wrinkly and leathery. But someone who’s gone a bit ancient, what’s the difference?
Jane - As we all get more ancient we will get more wrinkly and our skin will be soft and less vibrant looking - it’s just what happens. So we lose some thickness to our skin as we get older; we get drier because our grease glands stop working quite so well, so we look a bit duller and definitely saggier.
Chris - If you pinch the back of your hand, for example. I remember doing this on my daughter earlier you just sort of raise the skin up like a tent, it immediately pings back in her. But in me… mmm it takes the return time, the relax time is a few seconds.
Jane - That’s right.
Chris - So why is that?
Jane - That’s your dermis that hasn’t got as much collagen and elastin as it did when you were younger.
Chris - And why is that?
Jane - That’s a natural ageing process but that’s magnified by the effects of the sun. So that’s one of the major effects of having a lot of sun exposure is we get collagen damage, and as we get older both collagen and elastin aren’t produced as much.
Chris - So when I go to a supermarket or chemist or something and buy and anti-ageing cream or something to make me look a bit younger, how do those things work?
Jane - If they work.
Chris - I suppose they’re defying the eye potentially aren’t they? But is it defying the eye, is it actually doing something physically to the skin?
Jane - They’ll do certain things, like every cream they’ll keep moisture in the skin so they’ll stop your skin looking dried up, and it’ll stop it drying up so much as the day goes on. They might have a little bit of shine to them, of course, if they contain greasy things so that dull look that can make you look older, you can lose that.
But the creams that are put forward as anti-ageing creams, there’s a bit of a debate as to how well they work because they really need to get down into the dermis to do something to that collagen and elastin, and they don’t do that as well on actual skin as they do in cell culture, for instance. The only constituent of anti-ageing creams that really has good evidence behind it are the retinoids - retinol.
Chris - They’re vitamin A like chemicals, aren’t they?
Jane - That’s right, similar to vitamin A. But put on the surface they do seem to go deep enough to produce a measurable effect on wrinkles.
Chris - And what is that effect? Are they encouraging the skin to what, make more elastic tissue; make more collagen?
Jane - Make more collagen, yes.
Chris - And that irons out the wrinkles a bit.
Jane - Yes. But, of course, but it’ll really only work when you’re using it. And the tests that are used to measure wrinkles are pretty detailed so whether you would notice a huge difference - probably not. You might notice a little difference to the end of treatment period with it.
Chris - And when one does slap on lots of makeup day, after day, after day relentlessly. Is there evidence that that’s bad for you? Does that age, harm, or damage the skin or does it not make any difference?
Jane - Well, as long as you don’t react to the makeup you’re putting on - you don’t develop an allergy to it, which is always possible. And as long as it’s not a drying, dehydrating effect on the skin then there should be no long term problems. For makeup, on other thing you can sometimes do if it’s a really heavy sort of concealer makeup it can bring up acne spots but otherwise should be no long term damage.

54:21 - Why do my Wellies feel heavier in water?
Why do my Wellies feel heavier in water?
Sam Brown asked Professor Colm-cille Caulfield from Cambridge University to wade in with an answer to Daniel's question...
Colm-cille - Think of a hat with a square rigid brim of 10 centimetres by 10 centimetres. When we do the calculations we find roughly a 100 kilograms of atmosphere is pressing down on that hat. It sounds like a lot, but we are used to it and so we don’t typically notice. But what we are actually strongly sensitive to are changes in pressure. Our ears can pop when we go up a hill and we can experience discomfort as a plane lands and pressure equalises...
Sam - To answer our question from Daniel there are three key points we must keep in mind…
Colm-cille - Firstly water is much denser than air, so pressure changes more rapidly with depth. Just 10 metres depth of water exerts a pressure roughly equivalent to the entire atmosphere.
Sam - That explains why submarines need to be sturdily built.
Colm-cille - Secondary, when you wear wellington boots, they hopefully keep you dry and so there is always a layer of air around your legs and feet. Anywhere where there is air in contact with skin, the skin will be feeling atmospheric pressure.
Finally, wellington boots are flexible and so can be affected and bend due to differences of pressure on the inside and outside.
So with bare legs in water, the water pressure is felt uniformly around the skin. The pressure variation is down the leg and is gradual so you don’t notice anything except perhaps where your legs break the surface.
Now consider the way that pressure changes around the boot. Over the depth of the puddle it changes much more rapidly in the water outside, than the air inside. If the puddle is deep enough, eventually, the pressure difference will be big enough to cause the boot to buckle and the rigidity of the boot will shift the forces around, squeezing your legs and toes in certain places. It is this contrast in where the boot touches and where it doesn’t that we notice.
Sam - So there you have it. As for what we can do about it? Maybe try wearing chunky socks next time to keep the wellies from buckling inwards.








 crystal")

Comments
Add a comment